Implants and prosthetics for the ageing patient

Dr. Volker Bonatz, M.Sc. M.Sc.
- Dr. Volker Bonatz received his dental education at the Christian-Albrechts-University of Kiel, Germany. He then gained diverse experience during his residency, serving at the Wilhelmshaven Naval Medical Corps and in various specialist practices.
- He earned a Master of Science (M.Sc.) in Oral Surgery/Implantology in 2010, and a Master of Science (M.Sc.) in Aesthetic Reconstructive Dentistry in 2013.
- He speaks at conferences in Germany and internationally on implantological and prosthetic topics. He is also a member of the German Society of Oral Implantology (DGOI).
- Dr. Bonatz operates a private practice in Landau, specializing in implantology and aesthetic- functional treatments. His approach focuses on providing patients with aesthetically pleasing and long-lasting functional solutions, carefully tailored to each individual‘s manual dexterity and financial considerations.
Anamnesis
A 70-year-old patient sought treatment for discomfort in the right mandible, specifically in an area where a bridge had been in place for approximately 30 years. We found that the mesial bridge abutment at tooth 45 was subcoronally destroyed. Additionally, tooth 47 exhibited tenderness when pressure was applied to the bite block. Given the patient‘s age and the condition of the jawbone, we aimed to avoid augmentation. Instead, our treatment plan involved placing particularly narrow implants in the atrophied areas. Due to the absence of an antagonist tooth, it was determined that replacing tooth 47 with a third implant was unnecessary.
Clinical casebook
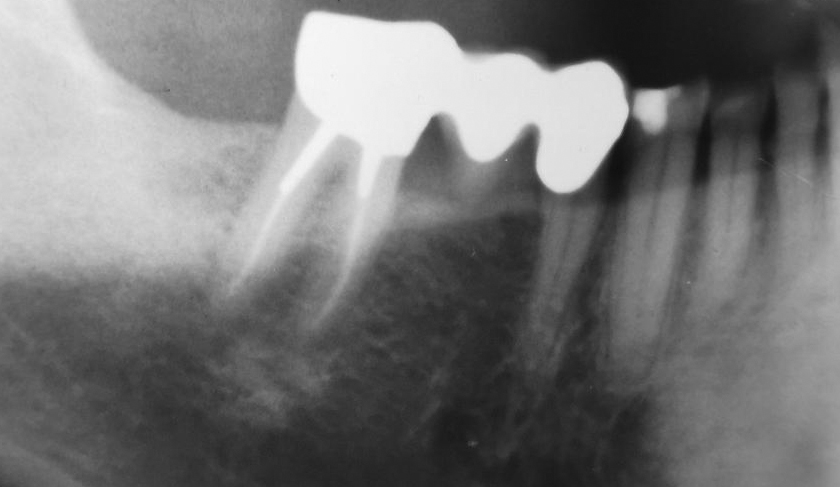
Initial situation: a subcoronally destroyed mesial bridge abutment 45 and a tooth 47 with a pressure sensitive bite block. An atraumatic and extremely bone-preserving tooth extraction followed. The alveolar walls were almost completely preserved.
Insertion: at 45 a 12 mm long BioniQ Plus implant with Ø 2.9 mm and at 46 an equally long implant with Ø 3.5 mm. Both implants have a pronounced machined neck to prevent plaque accumulation over time.
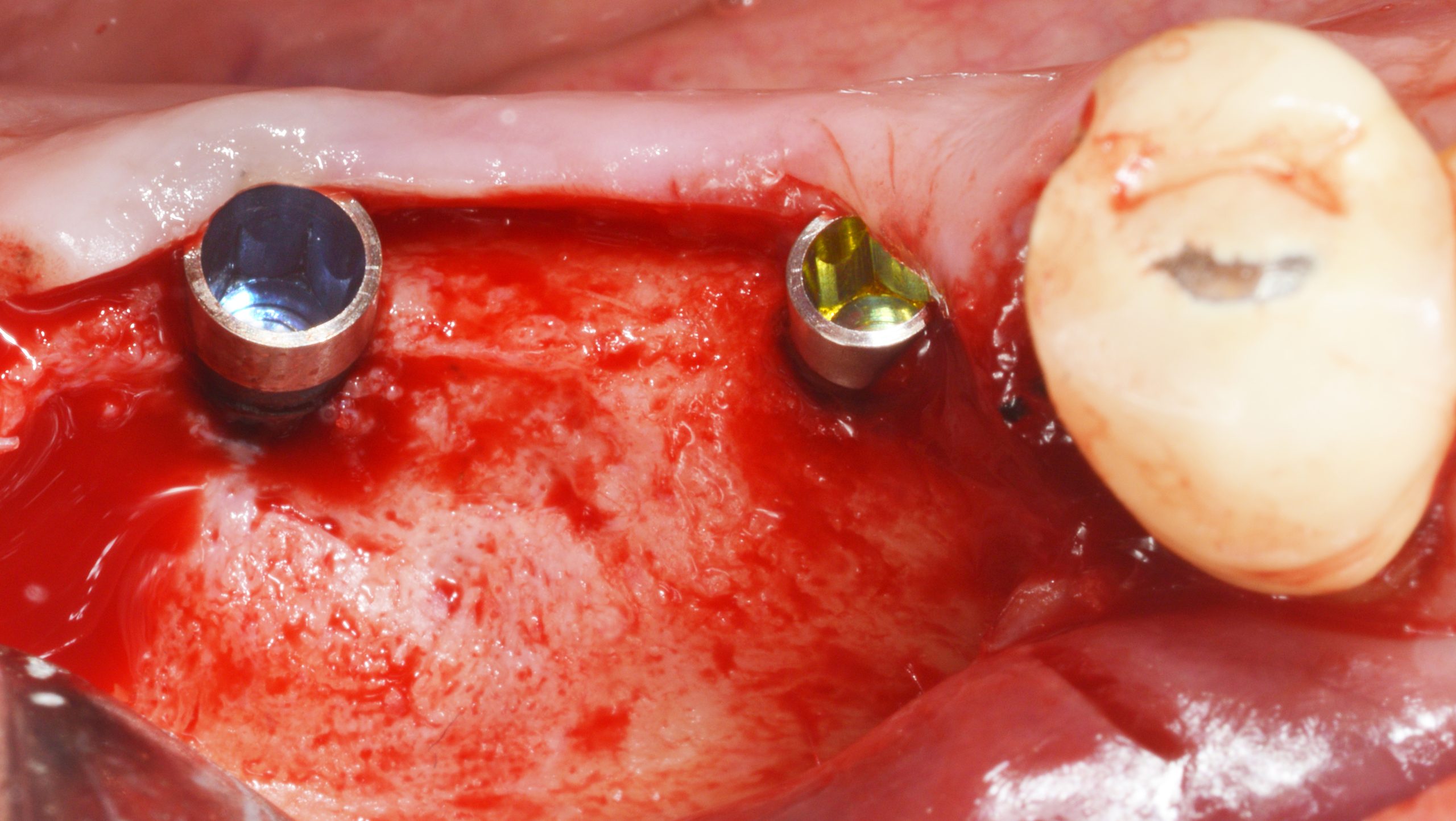
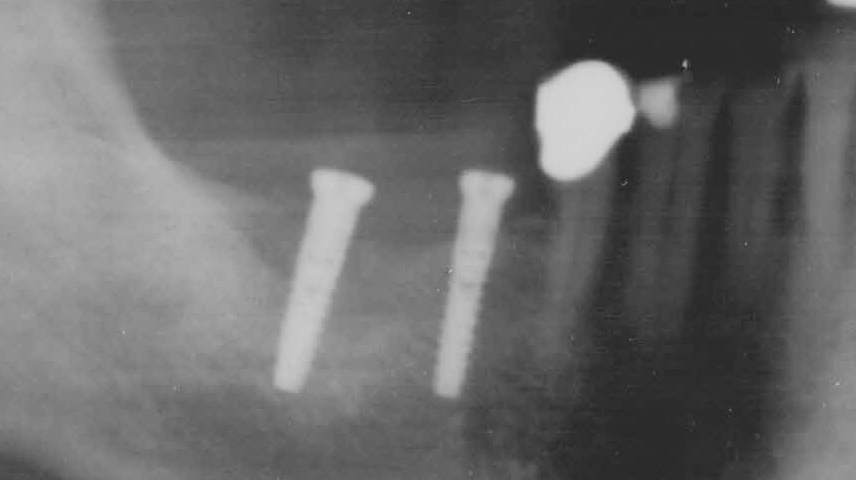
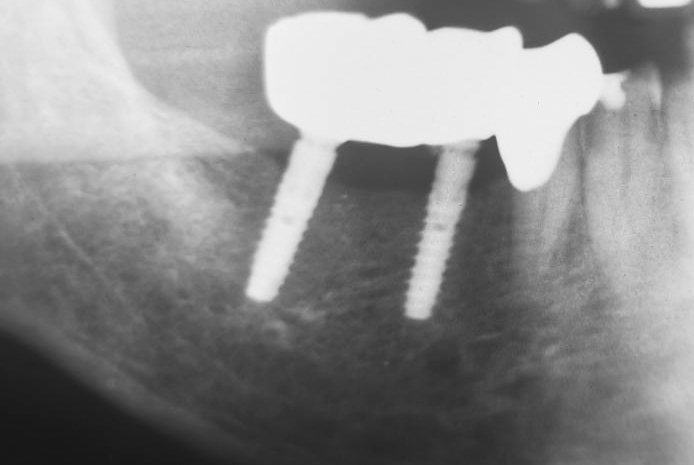
The implants were inserted with primary stability and with the machined surface up to bone level. The X-ray check confirms that the BioniQ Plus implants inserted are of sufficient length.
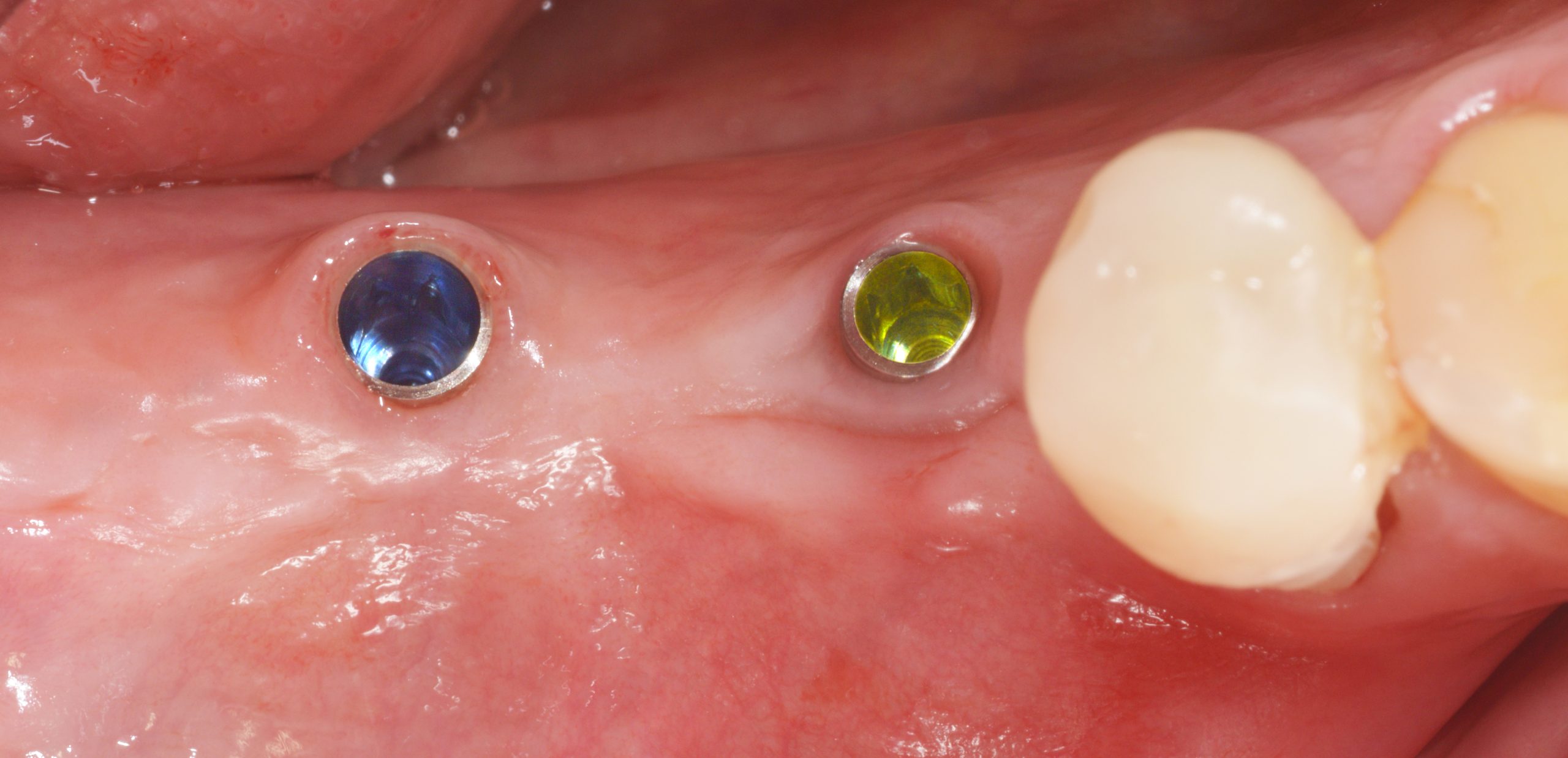
During open healing, cleaning checks were carried out with instructions to also clean the cover screws using special brushes to ensure an inflammation-free peri-implant gingiva.

Due to the open healing, surgical exposure was not necessary. The Ostell was used to document the strength, which was well above 70 ISQ for both implants. Gingival conditions before the impression was taken were clean.
In the course of the treatment, the defective crown 44 was also redesigned. The implant fit was verified with an implant control splint to be on the safe side due to the very slight distortion that can never be ruled out when taking the impression.

Intraorally, the splint can be fitted tightly but without tension.

If possible, all implant prosthetics should be screw-retained to have quick “service access” in the event of bruxism-related screw loosening, for example. The master dental laboratory sandblasted the tried-in abutments.
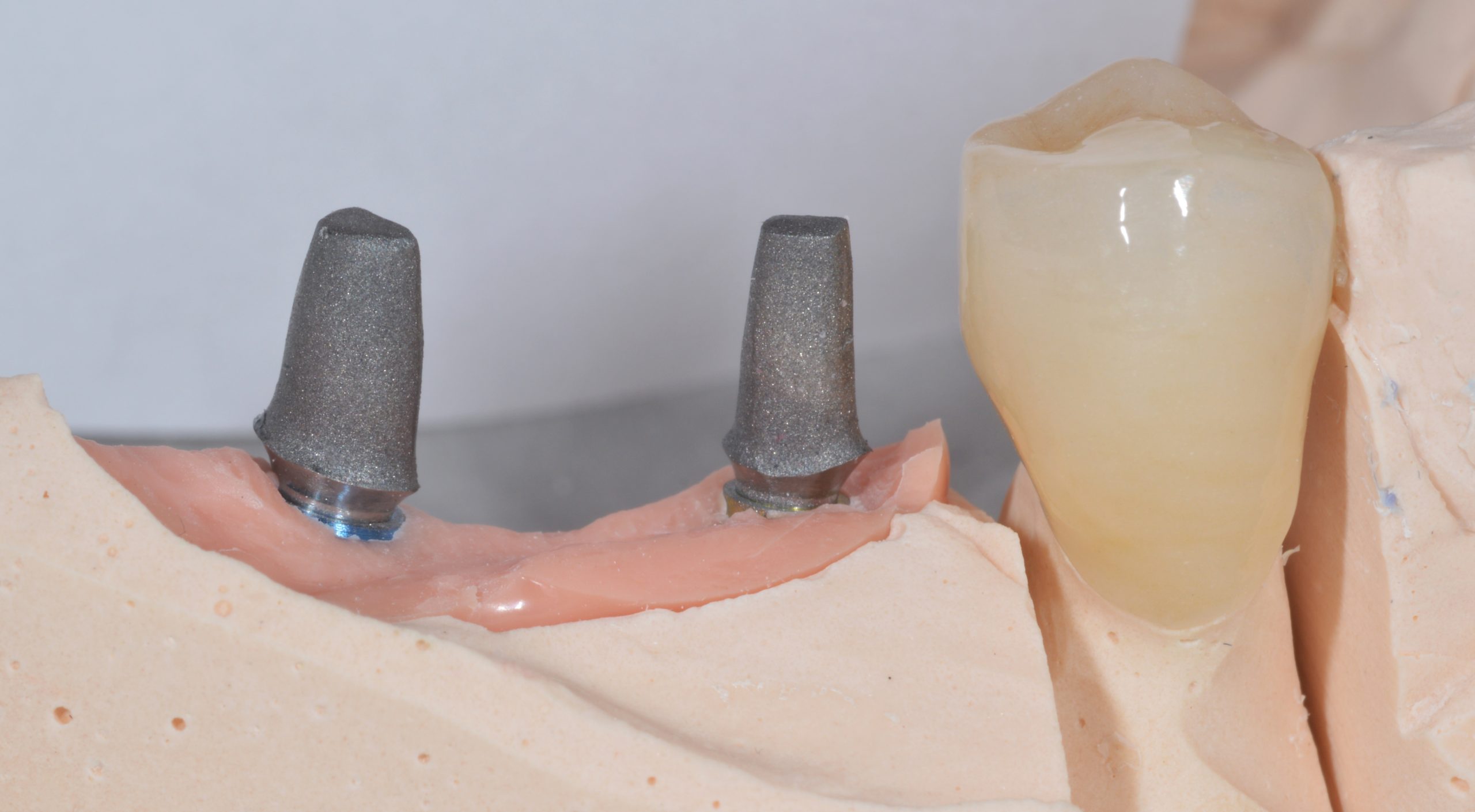
A ZrO2 block with two occlusal access channels was fabricated.

After the two abutments were tightened and filled over the screws, the ZrO2 block was bonded intraorally and the openings were then sealed with plastic material.

In addition, the dental technicians ensured a cleaning-friendly basal passage between 45 and 46. The handling of the interdental brushes was checked and the patient was instructed to attend a regular recall.

The X-ray 14 months later shows a stable peri-implant bone level, which may have increased distally to the 2.9 implant.
Here you can download clinical casebook